International Myositis Classification Criteria Project (IMCCP) Workshop
Held on November 11, 2005
MEETING SUMMARY
This document summarizes a meeting of available members of the Steering and Working
Committees of the International Myositis Classification Criteria Project who met on Friday
November 11, 2005 from 8:30 AM to 3:30 PM at the Washington Dulles Airport Marriott Hotel,
Dulles, Virginia (attendees listed in Appendix 1). The purpose of the meeting was to define
approaches and variables to be collected in a retrospective study to develop new classification
criteria for the idiopathic inflammatory myopathies and their subgroups.
In prior meetings, it was decided that this project is needed because of the lack of reliable
information on sensitivity and specificity of all current criteria sets, because of the many different
unvalidated criteria now being used, and due to the availability of novel technologies and
approaches today that offer new opportunities to revise our thinking and definitions of myositis. For
those who are members of the International Myositis Assessment and Clinical Studies Group
(IMACS) and who wish to view all the documents and slides presented at the IMCCP Planning
Meeting in 2004, see https://dir-apps.niehs.nih.gov/imacs/index.cfm?action=home.meetings
.
It was decided that a combined interdisciplinary effort addressing both adult-onset and childhood-
onset myositis would be ideal and that there should be two primary goals for the project:
I. Criteria should be developed for use by basic and clinical researchers that
distinguish the idiopathic inflammatory myopathies (IIM) from other major
mimicking conditions with high sensitivity and specificity; and
II. Criteria should be developed for use by basic and clinical researchers that
separate the major subgroups of the IIM from each other with high sensitivity
and specificity.
1. Introduction – Ingrid Lundberg, Chair of the Project, summarized the developments that led to
the current meeting emphasizing the growing split among different specialities in terms of how the
idiopathic inflammatory myopathies and their major subgroups are viewed and defined and how
this could lead to great difficulties in future meta-analyses and attempts to correlate findings from
one trial or study to another. She discussed the activities of the first Steering Committee held in
November 2004 that lead to this meeting. She also described current interest and joint funding by
the European League Against Rheumatism (EULAR) and the American College of Rheumatology
(ACR) to support these efforts to develop criteria that would be recognized by these and possibly
other groups.
2. Matthew Liang reviewed his background from previous work on development or revision of
criteria in other disorders and the general processes that would be followed during the meeting
and then led the Nominal Group Technique throughout the sessions.
3. Fred Miller reviewed the organization and conduct of the pilot study which retrospectively
collected data from 50 variables on 34 subjects with myositis and 14 subjects without myositis in
order to assess the availability and feasibility of collection of certain of these variables (see
Appendix 2). He then introduced the Nominal Group Technique and its advantages and how it
was going to be used at this meeting.
4. Variables were considered by Nominal Group Technique in the following categories:
A. Clinical Muscle Variables
B. Skin Variables
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
1
C. Other Clinical Variables
D. Laboratory Variables
E. Muscle Biopsy Variables
A common approach was used for each category: first, Tony Lachenbruch reviewed his statistical
analyses of the variables from the pilot study. Then Matt Liang, Ingrid Lundberg, Fred Miller or
Lisa Rider led the group in repeated round-robin fashion asking for possible additional useful
variables. Finally each member was given the opportunity to mark a set number of proposed
variables that should be eliminated from the list for a variety of reasons including:
a. They were likely to often be missing in the retrospective medical record review
b. They were difficult to define
c. They were redundant
d. They were too rarely endorsed
e. They were non-discriminatory
f. They were costly to obtain, either financially or due to inconvenience, or
g. They were likely to differ in various ethnic populations
The proposed variable list obtained by this process, and including those variables from prior
proposed and published criteria, needed to assess their sensitivity and specificity, is listed in
Appendix 3.
5. Fred Miller presented the subgroups proposed by the Steering Committee to include within the
umbrella rubric of idiopathic inflammatory myopathies and those diagnostic groups to include as
non-idiopathic inflammatory myopathies. Attendees added to the list of potential myositis
subgroups and non-myositis diagnoses. Following the meeting, however, the number of myositis
subgroups was restricted due to sample size considerations for the study (see G7 in Appendix 3).
6. Tony Lachenbruch gave a brief presentation of the general issues to consider in defining cases
and variables and listed some power analyses for our consideration of the number of cases to
study. These questions included: How many variables should we collect? In which way should we
choose patients and over what period of time? Subsequent discussions by members of the
Steering Committee resolved that 750 IIM cases (divided as evenly as possible among the IIM
subgroups below) and 500 non-IIM comparators (divided as evenly as possible among the non-IIM
diagnostic groups below) should be initially studied, with a first request for 5-10 cases of IIM and 5-
10 cases of non-IIM from each participant. Following the collection of data on these initial cases
(by either a paper form or by an Excel database), an assessment of these data will be made to
determine the number and types of additional cases that may be needed to achieve adequate
power to complete the study. The criteria for choosing subjects for the study, in order of priority,
should be:
i. The subject has been diagnosed for at least 6 months to allow for an adequate
assessment of response to corticosteroid or other immunosuppressive therapy
ii. The physician is certain of the diagnosis – only cases with known idiopathic
inflammatory myopathy or, as comparators, known non-IIM cases (but in which
myositis was considered in the initial differential diagnosis) are chosen
iii. The most complete data are available - >60% of all variables present
iv. The most recent cases are chosen first – these would likely result in more
consistent evaluations and therapy
7. Ingrid Lundberg then led the group in discussing the overall work plan for the meeting and
timeline for the project, in hopes that it could be completed in the next two years:
Oct. 2004 – First planning meeting held at NIH
Sept. 2005 – Pilot project performed on 50 variables
Early 2006 – Variables and project plans finalized, including glossary of the variables
Late 2006 – Complete data collection of initial 1250 pts
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
2
Late 2006 – Complete analyses of initial data to determine needs for additional data collection
Mid 2007 – Complete all data collection
Late 2007 – Completion of all data analyses
Late 2007 – Experts determine final proposed criteria and possible future plans
8. Ingrid Lundberg and Matthew Liang closed the meeting by defining some other aspects of the
process for the development of these criteria and future plans.
a. The next step was to summarize the meeting and preliminary variable list with
definitions of the variables and distribute this by email to the larger number of
experts interested in this project, but who could not all attend this meeting, for
their comments and suggestions. Members of the working and steering
committees represent many collaborative study groups and are encouraged to
involve their respective groups in the project.
b. A concern was raised that the participants in this project should represent
different specialties with a balance among disciplines and it is particularly
important that neurology is balanced with rheumatology. Furthermore, the
participants recruited so far represent North America, Mexico, Europe and
Australia, but additional representatives from Asia and South America are
particularly needed. The participants of the meeting were asked to nominate
other experts to be invited for the future work. A list of participants that have
accepted to participate in this project as well as nominated experts to be
contacted is attached as a separate file. This larger group would be invited to join
the International Myositis Classification Criteria Project, to vote on variables to
define the final list, and then contribute cases to the study. It is to be emphasized
that many of the current participants represent larger collaborative study groups,
including IMACS, ENMC, Muscle Study Group, European JDM Network, PRINTO
and CARRA. It is intended to engage a broad participation in the medical record
review from each of these and other collaborative groups. As a consequence of
the workshop we have also extended the Steering committee with one
dermatologist and two neurologists.
c. The process should include the development of an extensive glossary with
standardized nomenclature as the variables are finalized.
d. Different approaches to analyze the data were discussed including heuristic
methods, major and minor criteria lists, probable and definite criteria,
classification and regression tree (CART) approaches, regression methods,
random forests classification – or, if funds permit, a combination of these could
be used.
e. It may be useful to define a pathology subcommittee of at least 3 members to
blindly review muscle biopsies and record findings using a specified format.
f. Other as yet unresolved issues that will eventually need to be addressed include:
possible training to enhance consistency in use of terms and collection of data
elements; possible subcommittees for MRI, autoantibodies, biopsies and
immunohistochemistry studies, if funding for these projects is obtained; how to
handle missing data (EMG, biopsies etc.); how to address international ethics
issues (possibly use a central Institutional Review Board (IRB) in the U.S. and
ethics exemptions when possible for retrospective anonymized chart reviews);
which of multiple statistical approaches are best; data collection and validation
methods; approval or acceptance of the developed criteria by neurology,
dermatology and other academies and groups.
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
3
Appendix 1 - Steering and Working Committee Members of the International Myositis
Classification Criteria Project who attended the Workshop held on November 11, 2005.
NAME
EMAIL ADDRESS
WORKING COMMITTEE MEMBERS
VINAY CHAUDHRY [email protected]
LISA CHRISTOPHER [email protected]
MARY CRONIN [email protected]
KATALIN DANKO [email protected]
BRIAN FELDMAN BRIAN.FELDMAN@SICKKIDS.CA
IGNACIO GARCIA DE LA TORRE [email protected]
GERALD HENGSTMANN G.HENGSTMAN@NEURO.UMCN.NL
RENATO MANTEGAZZA RMANTEGAZZA@ISTITUTO-BESTA.IT
CHET ODDIS [email protected]U
PAUL PLOTZ [email protected]
ANGELO RAVELLI ANGELORAVELLI@OSPEDALE-GASLINI.GE.IT
MICHAEL ROSE [email protected]
IRA TARGOFF [email protected]
JIRI VENCOVSKY [email protected]
VICTORIA WERTH [email protected]U
ROBERT WORTMANN ROBERT-WORTM[email protected]
STEERING COMMITTEE MEMBERS
ANTHONY AMATO [email protected]
PETER LACHENBRUCH [email protected]
MATTHEW LIANG MLIANG@PARTNERS.ORG
INGRID LUNDBERG (CHAIR) [email protected]
FRED MILLER [email protected]
CLARISSA PILKINGTON C.PILKINGTON@BTCONNECT.COM;
LISA RIDER [email protected]IH.GOV
OBSERVER FROM THE MYOSITIS ASSOCIATION
THERESA CURRY [email protected]
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
4

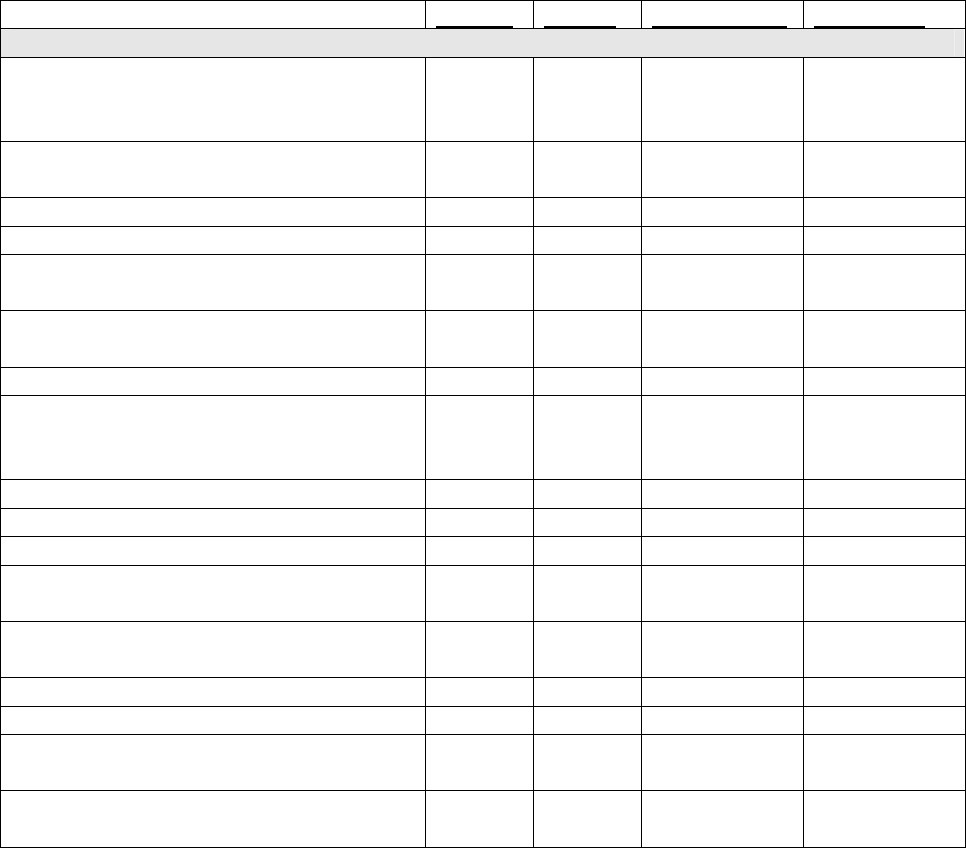
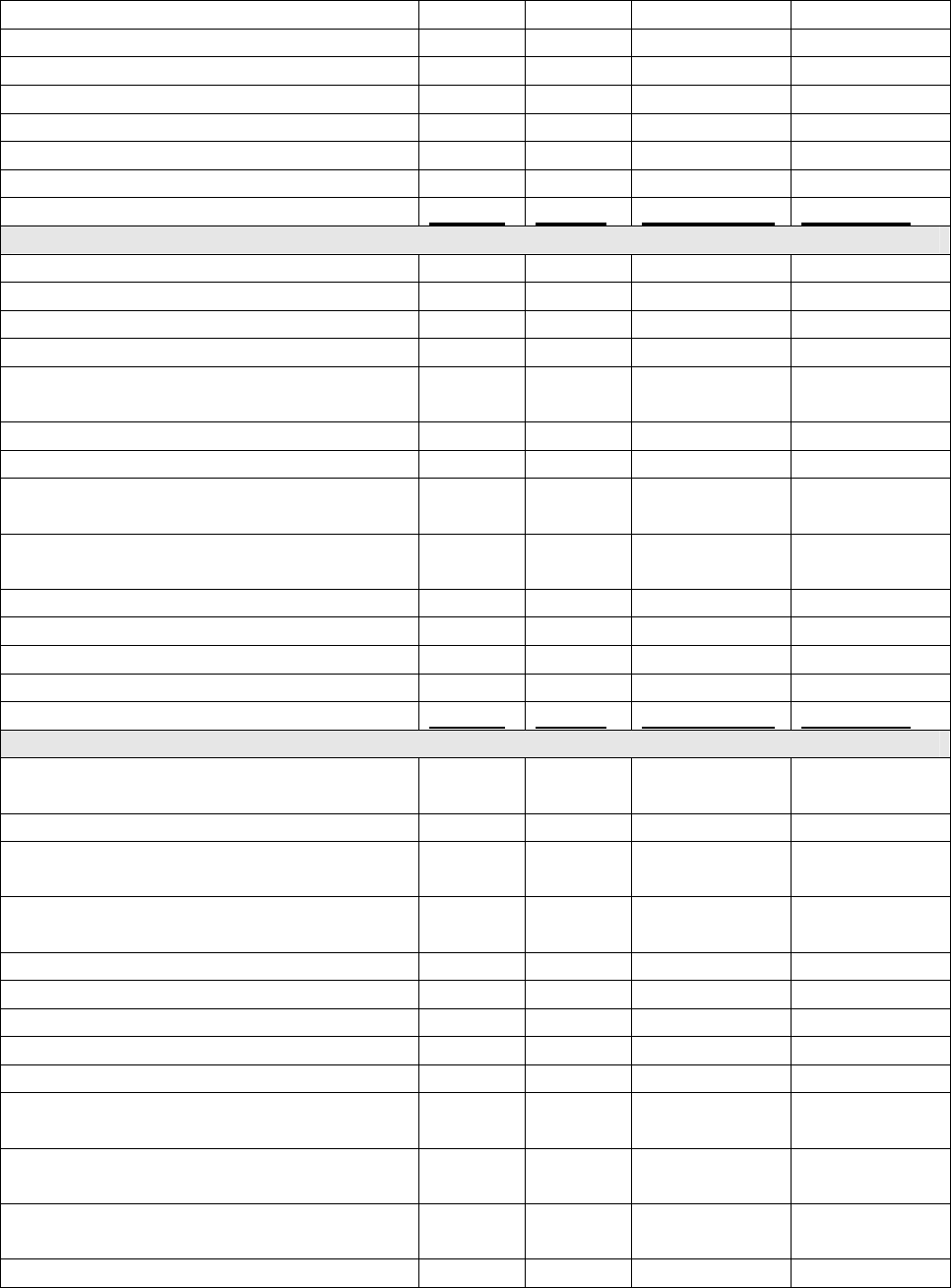
Appendix 2. Pilot study on 50 variables from 34 subjects with myositis and 14 subjects without
myositis to assess variable availability from retrospective chart review.
Category Variable
IIM %
(N)
present
IIM
%(N)
missing
Not IIM
%(N)
present
Not IIM
%(N)
missing
Sensitivity% Specificity%
Clinical
Muscle 1M Weakness, Prox UE 97 (33) 0 71 (10) 0 97 29
2M Wrist or FF weakness 56 (19) 6 (2) 2 (15) 1 (7) 56 79
3M Wrist/FF > shoulder abduct 18 (6) 9 (3) 7 (1) 14 (2) 18 79
4M Weakness, Prox LE 97 (33) 0 50 (7) 0 97 50
5M Hip abductor weakness 88 (30) 6 (2) 43 (6) 7 (1) 88 50
6M Weakness distal LE 41 (14) 0 21 (3) 14 (2) 41 64
7M Knee extensor weaker than hip 18 (6) 6 (2) 7 (1) 14 (2) 18 79
8M Neck flexor weakness 85 (29) 0 43 (6) 0 85 57
9M Neck extensor weakness 21 (7) 21 (7) 7 (1) 21 (3) 21 71
10M Symmetric weakness 85 (29) 0 57 (8) 7 (1) 85 36
11M Muscle pain at rest 32 (11) 18 (6) 29 (4) 0 32 71
12M Muscle tenderness 35 (12) 9 (3) 7 (1) 7 (1) 35 86
13M Muscle atrophy distal forearms 18 (6) 3 (1) 0 0 18 100
14M Thigh atrophy 32 (11) 3 (1) 0 0 32 100
Clinical Skin 1S Heliotrope 38 (13) 0 0 0 38 100
2S Gottron's papules 44 (15) 0
14 (2 DM
sine) 0 44 86
3S Erythema extensor surfaces 35 (12) 0 29 (4) 0 35 71
4S V-sign 21 (7) 0 7 (1)
0 21 93
5S Shawl sign 24 (8) 0 0 0 24 100
6S Calcification 9 (3) 3 (1) 0 0 9 100
7S. Periungual eryth, petech, telan, cutic
over
41 (14) 0 7 (1) 0 41 93
8S Raynaud's 18 (6) 3 (1) 29 (4) 0 18 71
Clinical
Other 1O Family history AD 26 (9) 9 (3) 28 (4) 0 26 71
2O Acute onset 71 (24) 3 (1) 43 (6) 0 71 57
3O Arthritis 47 (16) 0 43 (6) 0 47 57
4O Polyarthralgia 44 (15) 0 50 (7) 0 44 50
5O Sjogren's syndrome 3 (1) 0 7 (1) 0 3 93
6O Systemic sclerosis 0 0 7 (1) 0 0 93
7O MCTD 0 0 0 0 0 0
8O Rheumatoid arthritis 0 3 (1) 43 (6) 0 0 57
9O SLE 3 (1) 0 29 (4) 0 3 71
10O Autoimmune thyroid disease 12 (4) 18 (6) 7 (1) 42 (6) 12 50
11O Objective improvement strength p
corticoid 79 (27) 6 (2) 43 (6) 43 (6) 79 14
12O No improvement strength p corticoid 3 (1) 35 (12) 14 (2) 43 (6) 3 43
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
5

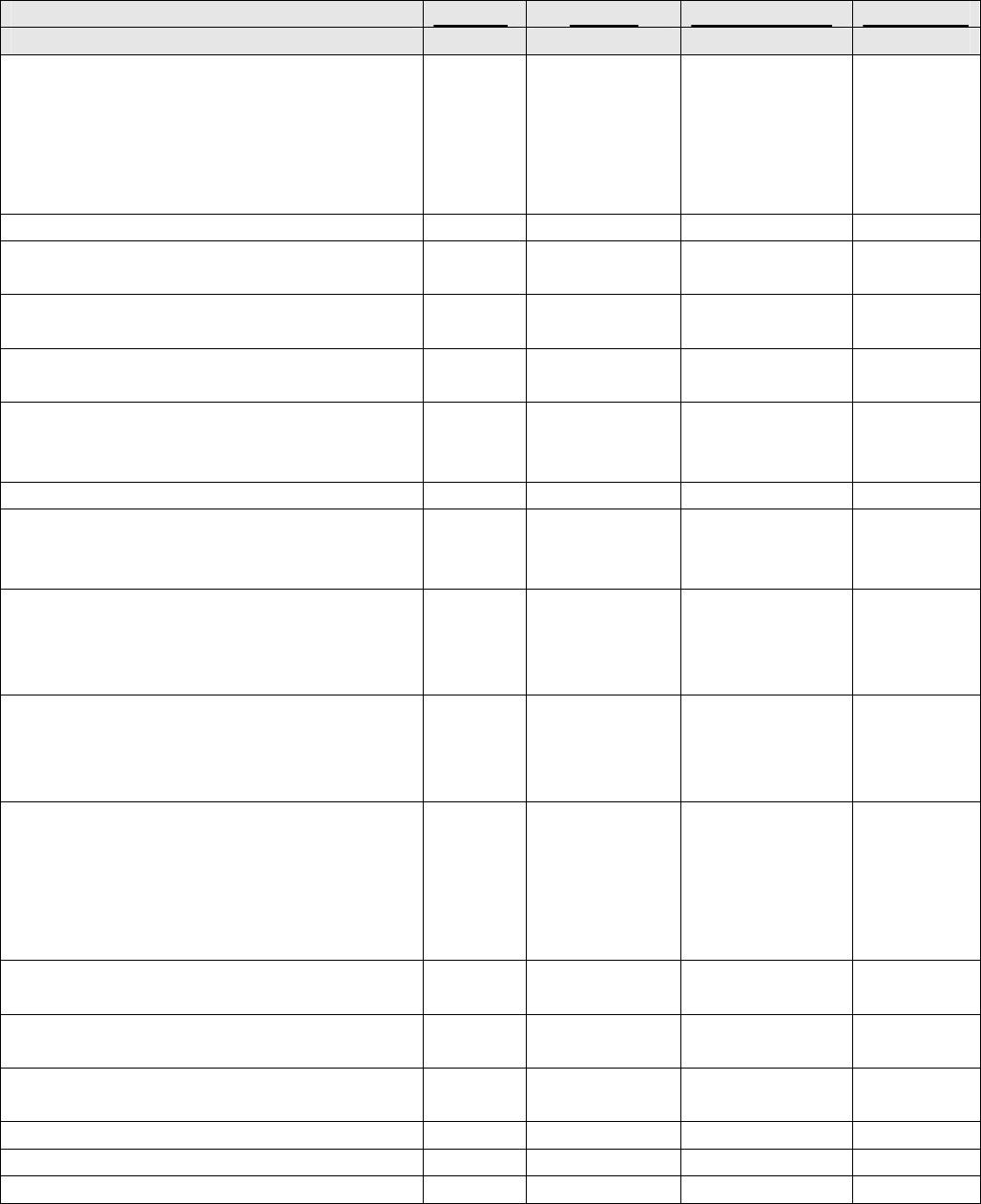
Appendix 2 (cont.). Pilot study on 50 variables from 34 subjects with myositis and 14 subjects
without myositis to assess variable availability from retrospective chart review.
Category Variable
IIM %
(N)
present
IIM %
(N)
missing
Not IIM
%(N)
present
Not IIM
%(N)
missing
Sensitivity
%
Specificity
%
Laboratory
1L EMG c/w IIM 59 (20) 32 (11) 14 (2) 79 (11) 59 7
2L CK elevated 76 (26) 15 (5) 36 (5) 14 (2) 76 50
3L LD elevated 53 (18) 38 (13) 7 (1) 43 (6) 53 50
4L AST/SGOT elevated 65 (22) 24 (8) 29 (4) 29 (4) 65 43
5L ALT/SGPT elevated 59 (20) 15 (5) 29 (4) 14 (2) 59 57
6L Aldolase elevated 15 (5) 82 (28) 7 (1) 64 (9) 15 29
7L ANA + 62 (21) 12 (4) 50 (7) 14 (2) 62 36
8L Anti-Jo-1 autoantibody + 21 (7) 21 (7) 0 29 (4) 21 71
9L STIR/T2 MRI c/w inflammation 62 (21) 26 (9) 21 (3) 50 (7) 62 29
Muscle Bx 1B Inflammation & degen/regen on H&E 34 (25) 15 (5) 14 (2) 57 (8) 34 29
2B MHC I ag present on muscle fibers 21 (7) 76 (26) 0 92 (13) 21 7
3B Non-necrotic fibers surr/invaded by
MNC 44 (15) 15 (5) 7 (1) 57 (8) 44 36
4B Endomysial MNC infiltrates 65 (22) 15 (5) 21 (3) 57 (8) 65 21
6B Perimysial MNC infiltrates 18 (6) 35 (12) 7 (1) 57 (8) 18 36
7B Perifascicular atrophy 21 (7) 15 (5) 0 57 (8) 21 43
8B Rimmed vacuoles 12 (4) 32 (11) 0 57 (8) 12 43
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
6
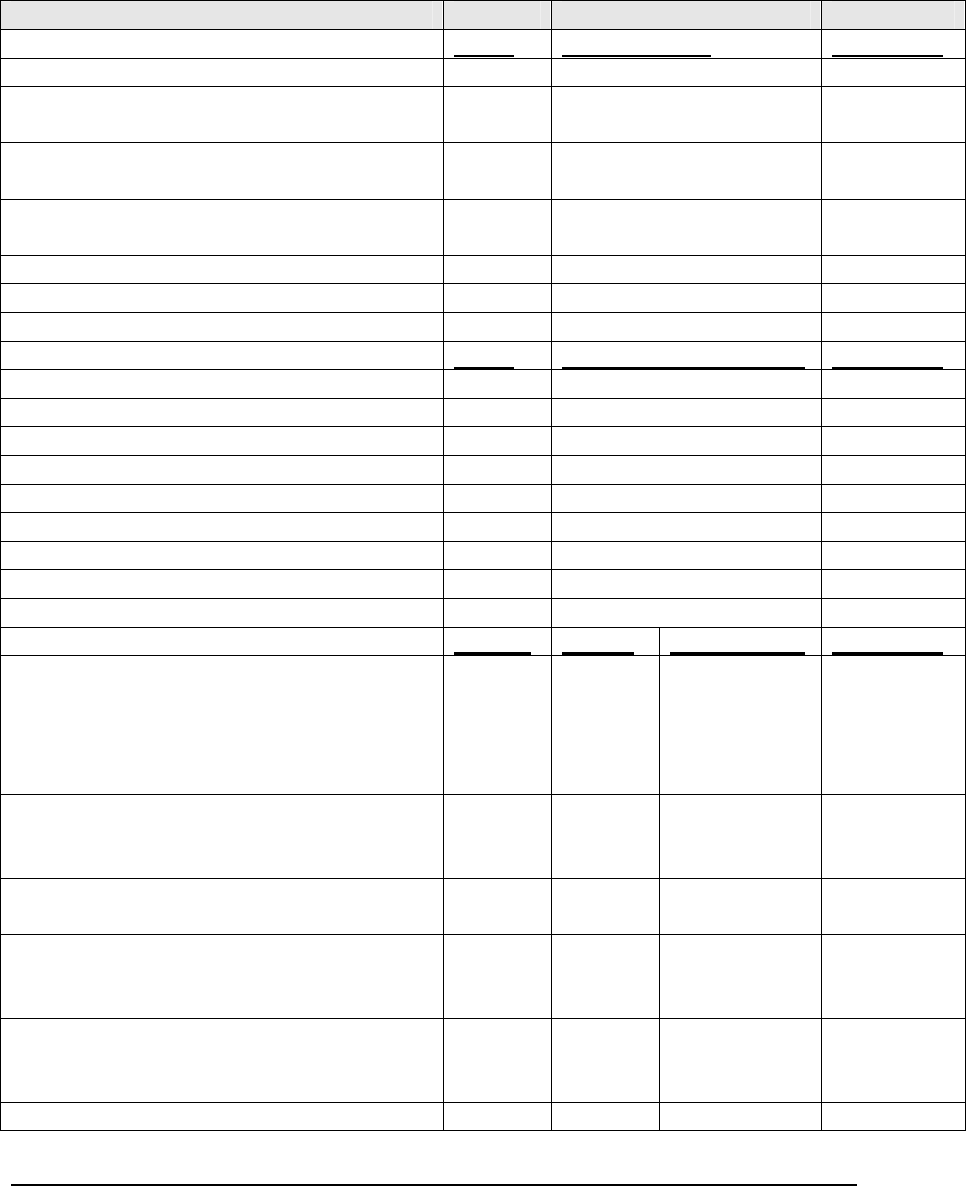
Appendix 3
Development of Classification Criteria for the
Idiopathic Inflammatory Myopathies and their Major Subgroups
Proposed Data Collection Form and Preliminary Variable List for Comment
Variables in italics are from prior proposed criteria and are needed to assess their
sensitivity and specificity
In reviewing patients please use the following criteria for selecting cases for submission:
i. The subject has been diagnosed for at least 6 months to allow for an adequate
assessment of response to corticosteroid or other immunosuppressive therapy
ii. The physician is certain of the diagnosis – only cases with known idiopathic
inflammatory myopathy or, as comparators, known non-IIM cases (but in which
myositis was considered in the initial differential diagnosis) are chosen
iii. The most complete data are available - >60% of all variables present
iv. The most recent cases are chosen first – these would likely result in more
consistent evaluations and therapy
GENERAL INFORMATION
G0. IRB or Ethic’s Committee approval identifier and date of approval:
G1. Clinician submitting case:
G2. Case identifier/number:
G3. Gender: □ Female
□ Male
G4. Age at onset: (of first symptom assumed to be related to the disease
G5. Age at diagnosis
G6. Ethnicity: □ Of European descent
□ Of African descent
□ Of Asian descent
□ Of Native American descent
□ Of Pacific Island descent
□ Of Mixed descent
□ Unknown
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
7
G7. Study diagnosis and onset (adult onset = age >17) according to the clinician (check only one
diagnosis):
Idiopathic Inflammatory Myopathy (IIM), adults or children:
Myositis Onset: adult □ or childhood □
□ Polymyositis
□ Dermatomyositis
□ Inclusion body myositis
□ Non-specific myositis
□ Immune-mediated necrotizing myopathy
NOT Idiopathic Inflammatory Myopathy (Not IIM), adults or children, but in which the
diagnosis of idiopathic myositis was considered in the differential diagnosis:
Disease Onset: adult □ or childhood □
□ Non-inflammatory inclusion body myopathy
□ Dystrophy, specify diagnosis
□ Metabolic myopathy, specify diagnosis
□ Mitochondrial myopathy, specify diagnosis
□ Drug or toxin associated myopathy, specify diagnosis
□ Infectious myopathy, specify diagnosis
□ Endocrine myopathy, specify diagnosis
□ Other Neuromuscular disease, specify diagnosis
□ Other Rheumatic disease, specify diagnosis
□ Other Dermatologic disease, specify diagnosis
G8. Basis for study diagnosis (check and explain in detail all supporting reasons):
□ Muscle weakness
□ Muscle biopsy abnormalities
□ Elevated muscle enzymes
□ EMG abnormalities
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
8
□ Rashes
□ Other, specify
G9. Clinicia
n’s additional comments on the case:
G10. Other diagnoses in this case:
□ Hypothyroidism
□ Hyperthyroidism
□ Type I diabetes
□ Rheumatoid arthritis
□ Juvenile Rheumatoid arthritis
□ Systemic lupus erythematosus
□ Systemic sclerosis
□ Multiple sclerosis
□ Other, specify
Present
Absent Not available Comments
Clinical Muscle Variables
1M. Objective symmetric weakness,
usually progressive, of the proximal
upper extremities
2M, Objective shoulder abductor
weakness
3M. Objective elbow flexor weakness
4M. Objective elbow extensor weakness
5M. Wrist and finger flexors are weaker
than shoulder abductors
6M. Wrist flexors are weaker than wrist
extensors
7M. Objective finger flexor weakness
8M. Objective symmetric weakness,
usually progressive, of the proximal
lower extremities
9M. Objective hip flexor weakness
10M. Objective hip abductor weakness
11M. Objective knee extensor weakness
12M. Knee extensors are as weak or
weaker than hip girdle muscles
13M. Objective muscle weakness of
distal lower extremities
14M. Objective axial weakness
15M. Objective neck flexor weakness
16M. Neck flexors are weaker than neck
extensors
17M. Proximal muscles are weaker than
distal muscles
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
9
18M. Muscle pain at rest
19M. Muscle tenderness
20M. Muscle atrophy of distal forearms
21M. Muscle atrophy of thighs
22M. Scapular winging
23M. Involuntary muscle movement
Present Absent Not available Comments
Skin Variables
1S. Heliotrope rash
2S. Gottron´s papules
3S. Gottron’s sign
4S. Erythema of the neck (V-sign)
5S. Erythema of the back of neck and
shoulders (Shawl sign)
6S. Periorbital edema
7S. Linear extensor erythema
8S. Cutaneous, fascial or muscular
calcification
9S. Periungual erythema or nailfold
capillary abnormality
10S. Cuticular overgrowth
11S. Mechanic’s hands
12S. Facial erythema
Present Absent Not available Comments
Other Clinical Variables
1O. Family history of autoimmune
disease
2O. Family history of muscle disease
3O. Subacute onset (weeks to several
months) of symptoms
4O. History of episodic weakness
associated with exercise or fasting
5O. Arthritis
6O. Polyarthralgia
7O. Unexplained Fevers
8O. Interstitial lung disease
9O. Peripheral neuropathy
10O. Dysphagia or esophageal
dysmotility
11O. Objective improvement in strength
after corticosteroid therapy
12O. Objective improvement in strength
after other immunosuppressive therapy
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
10
Present Absent Not available Comments
Muscle Biopsy Variables
1B. Necrosis of type I and type II muscle
fibers, phagocytosis,
degeneration/regeneration of myofibers
with variation in myofiber size, endomysial,
perimysial, perivascular or interstitial
mononuclear cells (MNCs)
2B. Perifascicular atrophy
3B. Non-necrotic fibers surrounded and
invaded by MNCs
4B. MHC Class I antigen present on
scattered muscle fibers
5B. Endomysial inflammatory cells
surrounding, but not invading, myofibers
6B. Endomysial CD8+ cells surrounding
myofibers with MHC Class I expression on
myofibers
7B. Vacuolated muscle fibers
8B. Intracellular amyloid deposits or 15-18
nm tubulofilaments by electron microscopy
(EM)
9B. Many necrotic muscle fibers as the
predominant feature. Inflammatory cells
are sparse; perimysial infiltrate is not
evident.
10B. Rimmed vacuoles, ragged red fibers,
or cytochrome oxidase-negative fibers that
would suggest inclusion body myositis
(IBM)
11B. Membrane attach complex (MAC)
depositions on small blood vessels, or
reduced capillary density, or
tubuloreticular inclusions in endothelial
cells on electron microscopy, or MHC-1
expression of perifascicular fibers
12B. Endomysial mononuclear cell
infiltrates
13B. Perivascular mononuclear cell
infiltrates
14B. Perimysial mononuclear cell
infiltrates
15B. Fatty replacement of muscle
16B. Glycogen or fat vacuoles
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
11
Laboratory Variables
Value Normal range Comments
1L. Serum creatine kinase (CK) activity
2L. Serum lactate dehydrogenase (LDH)
activity
3L. Serum aspartate aminotransferase
(ASAT/AST/SGOT) activity
4L. Serum alanine aminotransferase
(ALAT/ALT/SGPT) activity
5L. Serum Aldolase activity
6L. Erythrocyte sedimentation rate (ESR)
7L. C-reactive protein (CRP)
Value Normal range (method) Comments
8L. Anti-Jo-1 autoantibodies
9L. Other myositis-specific autoantibody
10L. Anti-nuclear autoantibodies (ANA)
11L. Other autoantibodies
a. Ribonucleoprotein (RNP)
b. La
c. Ro
d. Smith (Sm)
Present Absent Not available Comments
12L. Electromyogram (EMG) - Increased
insertional and spontaneous activity in the
form of fibrillation potentials, positive
sharp waves, or complex repetitive
discharges
13L. EMG - Morphometric analysis reveals
the presence of short duration, small
amplitude, polyphasic MUAPs
14L. Electrocardiogram (EKG)
abnormalities consistent with myositis
14L. Muscle inflammation on STIR or T2-
weighted magnetic resonance imaging
(MRI)
15L. Muscle abnormalities on T1-
weighted MRI scanning consistent with
myositis
Other features important in making the diagnosis not listed above – please specify:
Summary of the International Myositis Classification Criteria Project Workshop held 11/11/2005
12
